

Advances in acute diseases
However, it is not so well known that leukemias can be very varied, and if we begin to classify them, we will first distinguish two large groups: those acute or those that kill in the short term and those chronic or those that evolve in the longer term. This time, because the most hopeful advances have been made in recent decades in this disease, I will refer to acute leukemias, and especially to a type that appears in children: acute lymphoblastic leukemia.

Recently the results obtained in the treatment of this disease in the last 30 years have been published by the St. Jude Children’s Research Hospital in the United States and I consider it interesting to offer supervision. From 1962 to 1988 1,702 children under 18 years of age with acute lymphoblastic leukemia have been treated with 11 different treatment protocols. However, we can group the following protocols into 4 groups:
- Lot A: It consists of 4 protocols used between 1962 and 1966. At that time with chemotherapy the malignant cells of the blood disappeared.
- Lot B: Formed by 5 protocols used between 1967 and 1979. With the recurrence of the disease in many children of the first group in the Central Nervous System, radiation therapy against this system began to be used.
- Lot C: Protocol used from 1979 to 1983. New chemotherapeutic drugs were used.
- Lot D: Protocol used from 1884 to 1988. We have a protocol that consists of maximizing the dose of drugs used at the beginning of treatment and combining those that complement each other. The duration of treatment is more than 2 years.
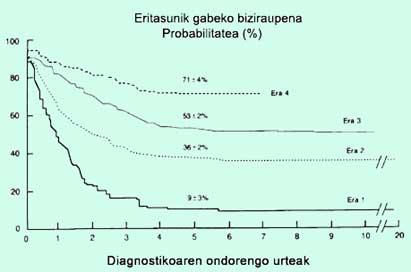
As can be seen in the figure, the proportion of children surviving 5 years after diagnosis without disease has continuously increased from group A to group D. Thus, if in group A we had only 9% without disease, in group B they were 36%, in group C 53% and in group D 71%. On the other hand, doctors know that in studies done to the child the survival of those who have certain symptoms is usually shorter, but we can also say that the survival of these children has increased a lot.
Giving an example of a child with a good prognosis, suppose a child is white of breed, 1 to 10 years old, with less than 50,000 white blood cells and group D. The probability of this child living without disease at age 5 is 86%. As an example of poor prognosis we can put the black child, less than a year or more than 10 years old, with more than 50,000 leukocytes and group D. The probability of disease-free survival at 5 years for this child would be approximately 60%.
In the first groups of different treatments, the greatest problems were due to relapse after the disappearance of the disease. The most common places for the recurrence of the disease were blood, central nervous system and testicles. In the last groups side effects of more compact and aggressive treatments begin to appear, especially infections and other cancers.
We have been able to analyze the long-term problems that have appeared in these children after an average clinical follow-up of 18 years. They have had 29 cases called solid cancers and 27 cases of acute myeloid leukemia. They may also present failures in body growth or development (especially because they may be lower) and alterations and deficiencies in intellectual and psychological development.
Although this work only refers to children, acute lymphoblastic leukemia can also affect adults and treatment results in them are less satisfactory. Although eradication of the disease is initially achieved in 70-80% of cases, at 5 years the proportion that survives without disease is 35%, half of what is achieved in children. Also, if this adult is over 50 or 60 years old, the results are even lower.
In some cases at risk of relapse, a bone marrow transplant may also be done, but we will leave this topic for another.
It is therefore clear that many children with acute lymphoblastic leukemia have been cured and efforts continue to improve outcomes. Let between a window open to hope and an increasingly bright light.
Note: In most European countries, including the Basque Country, similar results are obtained and there are no delays with the United States.
Zu idazle
Zientzia aldizkaria

