

Vegetable fiber

We will begin by recalling some general concepts about the structure of sugars or carbohydrates. The simplest unit of all sugars is monosaccharide, with a number of units that can range from one to one thousand. For example, glucose (C 6 H 12 O 6) is the sugar of the grape and has only one unit. Sucrose, the common sugar we have at home, has two monosaccharides and finally cellulose (a carbohydrate present in plants), from 8,000 to 10,000. Two types of monosaccharide bonds may appear: -glycosides and -glycosidic.
And there is the key, while the enzymes present in our organism attack the first link, do not do the same to the -glycosidic link. Because in food there are many compounds linked by glycosidic bonds, animals (and we of course) cannot take advantage of them directly. To combat it, there is a symbiosis between animals (including man) and bacteria, and microorganisms break this link and the animal can take advantage of the fractions of the large sugar molecule.
In humans, in our gut, both in the intestine, as in the ascending colon or in the distal part of the intestine, there are bacteria that break the -glycosidic bonds. However, the amount of cellulose they can break is very low.
Plant fiber is a very complex and broad term: they are remains of vegetables that are not attacked by human plates or that, in their elaboration, are attacked in less than 100%.
Fiber comprises the following products:
- Cellulose: It consists of glucose units between 3,000 and 10,000 units. It is the most abundant organic compound in nature. (1.4) having connections, the human being cannot take advantage of them. Not soluble in water because it has a linear structure. This chemical structure is very stable thanks to hydrogen bonds.
- Hemicellulose: We have 250 different products. Due to its complex composition we can distinguish between five and six distinct monosaccharides, some of which contain glucuronic acid and galaturonic acid. Xylose and, to a lesser extent, mannose, galactose, glucose and boughs stand out. Next to them and combined appear mananos and xylans. Between 15% and 20% of the wood materials of vegetables are hemicellulose. Its size is smaller than that of cellulose. The products inside the hemicellulose attach large amounts of water and some hemicellulose can fix cations, which causes irritation of the intestine and helps fecal excretion.
- Lignin: They are non-hydrocarbon derivatives of phenylpropane. Its molecular weight is 1500-4000 daltons.
It fixes a large number of bile salts, delays their absorption and prevents bacteria from acting on them in the digestive tract. According to recent studies, the influence of this molecule is evident in the reduction of colon cancer and cholesterol. - Pectin: its molecular weight ranges from 60,000 to 90,000. The main component is galacturonic acid and, in variable proportion, galactose, arabinosa, ramnosa, fucosa, etc... It is located in the intracellular openings of plant walls and plants. High water absorption capacity. It is present in many fresh vegetables and fruits, such as apples and their surfaces. Fixation of cations and bile salts and subsequent degradation of organisms. For this reason, in the Soviet Union it is integrated into the measure of resistance of workers working with heavy metals.
- Gums and mucilage: They are very branched compounds. Some contain glucuronic acid and others contain galacturonic acid (usually there is a mixture of both) and alternate xylose, arabinous and mannose. They
dissolve in water forming gels that are used as thickeners or as adhesive products (gum arabic). - Agar: It is extracted from seaweed and marine ears. It consists of mannose, xylose, glucose and glucuronic acid. We can distinguish two variants: agarose and agaropectin.
- Alginates: They are composed of manuronic acid and glucuronic acid. They are used in the pharmaceutical industry and as thickening agents and emulsifiers in the pastry industry.
- Phytic acid: It fixes large amounts of calcium (II)- and magnesium (II).
- Hydroxylated fatty acids.
Importance from a food point of view
- There are no enzymes to take advantage of fiber.
- Some products (pectin) are used thanks to bacterial symbiosis.
- The role of fiber is not to feed. So why does it exist in nature? Why as its consumption decreases increase some diseases such as colon cancer, diabetes, obesity, diaphragm gap, varicose veins, inflated, hemorrhoids, etc. ?

If an individual takes little fiber, it will defecate less times and also strives more than the one who consumes a lot of fiber. Abdominal pressure increases and as a result there is an interruption of the diaphragm, varicose veins, hemorrhoids, etc. will appear.
Normal meals are ironed in the first meter of the intestine. If the intestine is empty, the muscles that help defection are not active. If food leaves little residue, intestinal movements to get ahead are inert. The presence of a large fiber residue promotes intestinal movement by absorbing large amounts of water and reduces intestinal transit time. Upon reaching the colon hydrolysis occurs, releasing irritating acids and favoring their excretion.
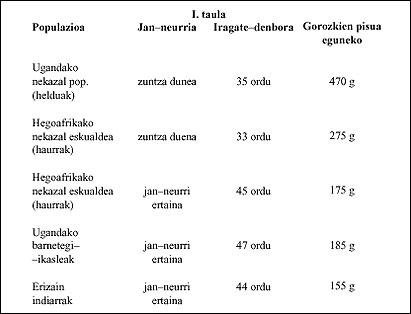
Transit time, as can be seen in Table I, is half in the case of fiber meals, compared to those without fiber. The weight difference is due to bound water and not to solid substances.
On the other hand, the more effort the abdominal pressure will be higher and the tension of the stool will increase. Therefore, the possibility of passing stool to the appendix and suffering appendicitis will rise considerably.
This is a dynamic problem, but metabolic problems also appear, as primitive populations have fewer diabetics.
It seems that fiber has a regulatory function, prevents the accumulation of large amounts of glucose in the body and that the consumption of fiber requires a longer time of gastric emptying, so the entry of sugars in the intestine is reduced, being its absorption less. Before this the insulin response will be less and therefore the possibility of suffering diabetes.
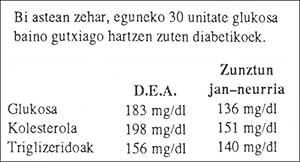
II. in the table (R.D.A.) The American Diabetes Organization provides some data on diabetics.
Patients who fed fiber after two weeks were able to stop taking insulin. Carbohydrates can be taken if eaten along with fiber.
The fiber content of a food decreases with frying and can sometimes be increased by cooking.
Another interesting aspect is that of infiltration and arteriosclerosis. There are few hells in populations with high fiber consumption. Fibers absorb cholesterol and bile acids from manufactured liver and cholesterol. The more bile acids synthesized by the liver, the lower the cholesterol. Bile acids are not excreted. On the distal side they are usually reused and returned to the liver. When this cycle works, the liver should only synthesize 10% of bile acids. If we interrupt the cycle, the liver should synthesize more bile acid and cholesterol will decrease.
This is done with cholestyramine in patients with familial hypercholesterolemia, but fiber does its job naturally. In addition, we must keep in mind that the shorter the passage time, the lower the amount of cholesterol absorbed. The relationship with cancer refers to the fact that bile acids synthesized by the liver are colic acid and kenodeoxycholic acid. However, in a sample of bile taken in the intestine we can find acids such as colic acid, kenodeoxycholic, deoxycholic, lithocolic and many derivatives formed by bacterial yherduence.
Intestinal bacteria contain enzymes that transform colic acid into deoxycholic, as well as kenodeoxycholic acid into lithocolic. The functioning of this enzyme system produces a number of products that irritate the colon. This effect, days later, produces the neoplastic transformation (cancer) of the last cells of the colon.

Fiber hinders bacterial activity, as it lightens transit and stops the formation of deoxycolic and lithocolic acids. On the other hand, the aforementioned acids will be more dissolved by bringing more water, being its action more reduced.
Bile is made up of about thirty substances, including cholesterol and bile acids. The first is soluble in bile, but not in water. An excessive increase in the concentration of deoxycholic acid will cause cholesterol precipitation and the formation of liver stones.
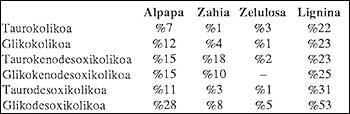
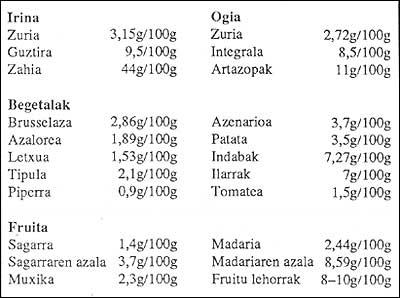
The fixation capacity of all these compounds varies according to food, III. as shown in the table .
III. The table data shows that lignin is the best protection against colon cancer.
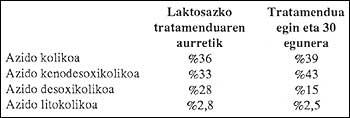
Lactulose is a laxative drug that inhibits the enzymatic activity of bacteria that break down bile acids. Therefore, it decreases the concentration of deoxycholic acid and the tendency to stone formation.
The alteration of pH in the fermentation of lactulose inhibits the enzymatic activity of the decomposition and raises cholesterol levels, discarding its precipitation and the formation of stones.
Zu idazle
Zientzia aldizkaria

