

Children born preterm
Among all animals, man is the only species capable of suffering a premature birth. If a lamb was born a week before what would correspond to him, it would die; the internal organs still cannot start working on their own. They are not completely mature. However, it seems that man has taken steps for a possible premature birth, since even before 40 weeks the child is able to survive outside the uterus.
The key to this peculiarity is the rapid maturation of the lungs. The lungs of a human being are prepared to start breathing on their own from week 34-35. Although until then the child has performed the breath through a placenta, it is able to fill and empty the lungs of oxygen. In fact, several weeks before birth, forming organs in the uterus. The blood he receives through his mother produces oxygen, but the child moves the chest as much as possible, putting and taking liquid into the lungs playing. Prepared for the birth.
Thanks to this privilege of our species, preterm children born from week 34 do not need great treatments. Just keep the incubator warm and collect the food and caresses of the mother. Real problems arise with those born before 34 weeks. And it is that they have to get underway with totally immature organs.
Neonatological resources

In these cases, medicine should help. However, it should be noted that neonatology is a special field within medicine: it is difficult to investigate with young children and progress very slowly.
The greatest challenge of neonatology has been to understand how the organs of the fetus develop in the uterus in order to imitate them in some way outside. Thus, in the final phase of pregnancy, it has been proven that the mother uses corticosteroids to get the baby's lungs completely, and now it is the same hormone that doctors use whenever they see that childbirth is premature. They give it to the mother when they realize that the lungs of the fetus mature as much as possible before childbirth.
But the possibility of breathing the lungs is more complex. Like a balloon inflated by the air, the lungs have a natural tendency to expel the air and they find it very difficult to catch air, they collapse. Therefore, the fetus must form a special substance to be able to breathe: surfactants.

The awareness that these substances contribute to the spread of alveoli has also been key in the care of preterm children. They are currently delivered to most children born before week 34.
Prenatal Surgery
Although the headache of the lungs is overcome, there is an insurmountable limit: the problem is that many times you can't know if the child has malformations until he is born. Since the heart of the mother, the kidneys, the lungs, has been used until birth, and in short all the organs, until the new organs of the child are born and started, it is not known whether they have developed well and if they are functional. If the malformations are not very visible.

To a certain extent, ultrasounds and x-rays have allowed detecting malformation prior to the baby's birth. But healing malformations is something else. A few years ago a pro-operation current emerged in the United States while children remain in the uterus, thinking that malformations could be minimized. But great controversies arose because many believe that the risk of termination of pregnancy was too high. Shortly after the hernias began to operate, it became clear that these courts caused the death of more children than to be cured.
Currently, simple cuts are made only in the kidneys. In fact, preventive intrauterine surgery has a future according to experts, but for the moment it is only science fiction.
Adolf Valls i Soler: “There are already those who advance with 400 grams”
Adolf Valls i Soler, Catalan researcher, is professor of Pedriatrics at the University of the Basque Country. His doctoral thesis was developed in the United States, where preterm newborns diagnosed lung diseases, and has been working for many years at Cruces Hospital. Your team investigates synthetic surfactants so that the lungs of the babies arrive as soon as possible. We found it working in the Neonatal Unit.
What is currently the minimum limit for a premature child to advance?
When I started working the border I was at 1,500 grams. Minor children died. But today the border has come down a lot: Children of 500 grams survive. And there are already those who advance with 400 grams. Imagine they are children between 24 and 25 weeks who have only done more than half of their pregnancy.
Do you have problems with this degree of maturity in the future?In the case of the Cruces Hospital, for example, at least 77% of newborns under 1,500 grams have taken a dose of corticosteroids to get the maximum grip of the lungs. Therefore, they have few problems at birth. The problem is that the medications they take also have side effects: for example, 20% of those who have ingested surfactants for lung maturation develop chronic lung diseases, although most are cured over time.
And where is the limit? Is it ethical to try to bring the life of any child forward, regardless of the degree of maturity?Well, it's hard to know where the limit of life is. If we see a child born very early, with less than 300 grams, then it is clear, there is nothing to do. We explain to his mother that before birth the child is not viable. When the lack of maturity of the fetus is too serious or has large malformations, there is no discussion. The decision is more complicated as this gravity decreases, when the organs are in the process of development. In these cases we have to decide case by case what is best for the child and his family. And, when it is too immature, extending life to the child is more than helping, acting without heart.
The most serious problem is that we are not sure. In adults it is easier to detect problems, but in neonatology it is not so simple. And there the problem begins. Doubts arise because medicine is not mathematical. In these cases we have to reach an agreement between all. We collect the opinion of other doctors, nurses and, of course, of the family. There is always negotiation and everyone agrees what to do.
In research there will also be ethical limits. In general, there are usually difficulties in trying drugs with people, and more if they are newborn children. In your group you investigate synthetic surfactants. How do you do these investigations?We experiment with laboratory animals, not with children. Before trying anything with children, with animals we do a lot of trials. The normal thing is that it is done with pigs, but in Euskal Herria it is much easier to get sheep. Therefore, as sheep are also suitable for research, we work with lambs. The pregnant sheep are caught and made a premature cesarean section, studying how the lungs of the lamb respond to surfactants. Also with synthetic surfactants we see that the lungs are able to arrive quickly.
And how do you decide to advance and test in children?
If we ask if it is ethical to conduct clinical trials with newborn children, people would say no in principle. Even more with these very young children. And if there is already a treatment in the market, that is, you can't experience. But when you don't have it and don't know which treatment is most appropriate, things change. In addition, there is a paradigm: when participating in clinical trials, the patient is better attended than ever. It does not matter whether you have been given a new drug or given a placebo; however, it is better than outside the trial. In the hospital, an effort is made to get the clinical trial well.
And when you propose to parents an opportunity like this, what is their attitude?Most of the time they tell us yes, they want to participate in clinical trials. Doctors are the ones we have the most, because we always want the most secure option. In addition, we must recognize that we do not know which treatment is most appropriate for the child. And that costs us to doctors.
Smaller brain areas
In the US. Children's brains have been analyzed and have shown that, eight years after preterm children were born, there are still smaller areas of cerebral cortex than normal children. The areas related to speech, reading, emotion and behavior.
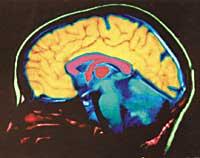
The difference is in the boys. They already knew that the early boys had difficulties with speech and studies, but they did not expect the difference in the brain to be so much, nor that after so long it was still evident. The girls have not noticed this difference in the brain, it seems that two X chromosomes give them some protection. It is also possible that the hormone levels that have in the blood before birth influence this difference.
Despite sex, researchers now aim for the brain: just as it has been possible to help preterm children develop the lungs, they also want it with the brain.
Human development Human development
Human development is not a 9 month process. It begins when the sperm and the egg come together, but ends in adolescence. And in this continuous process, childbirth is a small event. It is the time when we stop being ‘parasites’ of our mother.
The most critical moment in intrauterine development is the formation of organs, which occurs at the beginning of pregnancy, in the embryo phase. From there they only have to grow and mature.
Day 0 Between 200 and 300 million sperm start a journey to the egg. After several hours of long journey, a few will arrive, of which only one of them will get access to the interior. Week 1. The genetic information of both parents is reorganized and the cell division begins. The embryo adheres to the woman's uterus.
To see the full picture click here.
Zu idazle
Zientzia aldizkaria

