

Laparoscopy: surgery without abdominal opening
Introduction

Laparoscopy means seeing the inside of the belly by inserting the tube through the skin. It is not necessary to extend the stomach through a tube with a large wound. Laparoscopy was initially used as a diagnostic tool, as it was the only way to see the liver live without opening the belly to those with liver disease. But soon, by the hand of gynecologists, they began to be used in therapeutics and then some professionals are showing that it is a means for more and more actions. Operating through the tube instead of opening the belly with a scalpel to perform operations in the belly has two advantages: the first is that the patient has less physical trauma (due to the small wound) and the second, that the hospital stay is shorter, also reducing the cost of health.
History
Surgical intervention through laparoscopy, that is, through a tube, in recent years and with the help of technical advances, is the expression of a new way of proceeding that in the 1980s was being integrated in the field of surgery. This new position is based on the fact that the interventions are performed with the least possible trauma or surgical wound. In English he has been called minimally invasive surgery.
The first known laparoscopy was announced by Dr. Kelling in 1901. He used it in dogs and later Jacobeus in people in 1910. In the 1970s, gynecologists promoted laparoscopic surgery as a means of intervention and sterilization of women in the ovaries.
First we will briefly explain the development of the surgery and then the laparoscopic method. The breakthrough of surgery has its origin in the discovery of anesthesia, which took place in 1846. That year, the first known anesthesia was performed in the Massachusetts hospital, by the prestigious surgeon Gosset. That year we left the long night dominated by the clutches of pain and pain in the light. The path that had the pain closed until then was released and the places of the body that previously could not be studied, thanks to anesthesia, the surgeon had at his disposal.
The other discovery that surgery needed to make its big leap came two decades later. That was antisepsis and then asepsis. Although asepsis is a concept that today passed at the current level, the XIX. Until the end of the 20th century they did not use gloves or clean the intervention equipment. Unknown surgical sterilization. Due to lack of cleaning and sterilization, infections or infections after any surgery, high mortality was produced, constituting the next strong barrier of narcosis (anesthesia) for the advance of surgery.

With anesthesia and asepsis, in the fight against diseases, the surgeon set out to hidden territories undiscovered, proof of this is the shocking and successful history of surgery of the last hundred years. In the case of the belly, expanding the belly with the scalpel, we have come to operate all the organs that are inside until we reach the transplants.
Despite the advance of surgery, technological advances have not been left behind and have found ways to perform smaller interventions to achieve the same goal. This has meant a reduction in the need for the scalpel and a new approach in the world of surgery, mitigating aggression.
The most significant advances have occurred in the last two decades. Sample of this new attitude is what happened with kidney stones and urinary tract. Until 1980, if the stones or stones of the urinary tract that give rise to renal colic were not ejected spontaneously from the urine, they had to be removed opening the belly or the back part with a scalpel, needing a long period of post-operative recovery. But in 1980 they developed the method of external machaqueo of stones by invisible shockwaves, called lithotripsy.
This was a major change in urological surgery. The same base was thought to be applied to gallbladder stones, and although the first steps were successful, it has been confirmed that the machines prepared for this is a method of using a small percentage of gallbladder to operate. Although it is a method that can be used quietly in kidney stones, the gallbladder must meet specific conditions for it, being most important to be able to flow the gallbladder. Laparoscopy does not have this condition.
To operate inside the belly, some have managed to break the dogma of opening the belly with a large wound and have shown that some interventions can be complemented with tubes. And this is the story of laparoscopy. Initially, and as already mentioned in the introduction, laparoscopy began to be used by digestologists 20-30 years ago to see the liver.
It was used exclusively for diagnosis. It was later used in therapy by gynecologists and in 1971 the first publication appeared, in which 14 cases of pavements of ovarian and fallopian tubes were cured with laparoscopy. Gynecologists have worked the most in the field of therapeutic laparoscopy and use this method to associate tubal in women to achieve sterility, as well as in many other interventions. However, despite knowing these good results, in the digestive system, due to its peculiarities, therapeutic laparoscopy has not been applied to date.

In June 1987, the first cholecystectomy or withdrawal of the gallbladder from laparoscopy was carried out, the authors of which were the French chirurists. Cholecystectomy is the most common intervention in general surgery with general anesthesia. In the short term, from that date to the present, this technique has passed the ocean and is also being applied in the United States. The technique is still novel, but it seems to be of great future. In the Spanish State, and also in the Basque Country, some groups have begun to take their first steps and, as with everything new, some have announced that this is a method that can already extend to many operations, such as the healing of stomach ulcers and duodenum, the operation of interruptions, etc.
Recall that as a curious fact, the first known cholecystectomy in the world (operative removal of the gallbladder) was carried out by Dr. Langanbuch in 1882.
If it is laparoscopy, endoscopy cannot be omitted. It is also done through tubes, but in this case the tubes are inserted through natural holes: by the mouth to see the stomach, by the anus to see the intestine, or by the urethra of the penis and vagina to see the bladder and urinary tract. In laparoscopy the skin is pierced, inserting the tube through the skin.
Technical details
As has been said, the word laparoscopy means seeing the inside of the belly thanks to a tube inserted by the skin. Several tubes are used in therapy. For the removal of the gallbladder four tubes of 0,5 and 1 cm of diameter are used. For the introduction of the tubes a skin wound of one or half centimeters is performed. The technique of removing the gallbladder is explained below.
The tubes are rigid and their function is that for the tools that we are going to introduce inside the belly there is a step on the surface. The first cut is done to the navel, as it is aesthetically a place where nothing is detected. A special needle is inserted through it, the Veres needle, which is used to produce a pneumoperitoneum in the belly. Pneumoperitoneum consists of air entering the abdomen (usually CO 2 or carbon dioxide).

We could define the belly as a hollow full of organs between the walls. The space between the wall and the various organs (liver, spleen, even, intestine, etc.) is only apparent, as it is empty, like the chorizos that are packed into the vacuum. However, the entrance of air into this gap makes it a space between the wall and the intestine due to the occupation of the air. Therefore, the first thing to do when entering the tube is to introduce air to the peritoneal hollow.
When entering the first tube, as there is no space between the wall and the intestine, there is the risk of perforation of the intestine, but commercial houses have devised needles that respect the intestines through a set of pressure.
From the first cut of a navel we will enter besides air light and a camcorder, all for one centimeter of a tube. You get a good view of the air and light, taking care internally the entrance of the other three tubes to avoid discomfort when entering the inside of the belly. What we are doing inside the belly is seen on a television monitor. Therefore, it operates in front of this TV monitor. In the drawing you can see the location of the tubes.
Once the four tubes are inserted, accompanied by a clamp and scissor, the same steps must be followed as for the classical operation of the gallbladder. First the cystic is located and isolated, then the cystic artery, and before cutting it are tied with staples or metal clips.
Once the gallbladder is released from its junctions, once the small tubes found in blood jump with electric or laser saline, it goes outside. To facilitate its extraction, the inside of the gallbladder is vacuumed with a special vacuum cleaner. If possible, it leaves through a tube, but if it is not possible (because the gallbladder is large) it leaves directly from the surface section. The intervention ends with the suture of the superficial cuts, with four sufficient points.
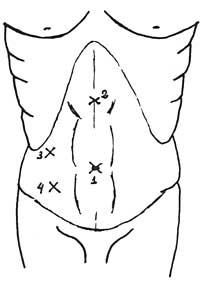
- From here the optics (light, video camera and wind input probe) are introduced. These tools are auxiliary. Clamps, coagulator, vacuum cleaner and scissors are introduced, which are handled by the operator. 4.- Tongs are inserted to keep the gallbladder in place and present it correctly to the one who is operating. Both tools belong to the wizard.
In a classical way, by the method called laparotomy, the removal of the gallbladder consists of cutting all the layers of the abdominal wall through a wound of about 12-15 centimeters in the belly to reach the interior, reaching the peritoneal hollow. We call this surgery open sky to differentiate it from laparoscopic.
With this technique called laparoscopy, and if there is no other problem, the patient is at home in 24-48 hours. Laparotomy or the classic method of ventral expansion take 6 or 7 days in the hospital.
Apparently, and this is the reason for rejection by those who do not know the technique, this technique seems more complicated and less secure compared to surgery performed with the open sky, especially because it seems that it is less or less visible. But this is not so, and to prove it must be taken into account that in the surgery that is done with the open sky, the eyes of the surgeon are about 1m from the area cut by the scissors and the light is two meters above the head of the operating room.
In laparoscopy, however, vision of the laparoscope is only a few centimeters or millimeters from the surgical site. The light is again at the same point and thus the force of light does not weaken. We must remember that light weakens according to the square of distance. In addition, if we place the eye and the TV camera on the laparoscope, we can see things enlarged on the monitor.
The works published by those who have so far removed the gallbladder with laparoscopy have yielded good results. The French Dubois, in 63 cholecystectomies, had problems or complications in 3 cases, which were cured without any problem with the enlargement of the belly.

The surgical material is special, but it is fixed in the conventional bases, finding scissors, clamp, rafa, electrocautery, etc. Right now a new microwave scalpel is being tested that cuts the parenchyma or tissues while respecting tubes and tubes.
With all this, although it is still early to predict how far things will come, you may think that laparoscopy has a foamy future.
The intervention time in the operation of the gallbladder with laparoscopy is longer than in surgery with open sky, but its reduction is achieved with the formation of this technique.
Zu idazle
Zientzia aldizkaria

