

Caffeine: a pleasure that can become a necessity

In recent years, there have been numerous doubts about the effects and mechanisms of caffeine. At the same time, contradictions have appeared about the ability of caffeine to create dependence. This article will analyze the results of the latest scientific research on consumption, dependence, abstinence syndrome, and the potential effects of this substance, in order to highlight the similarities and differences presented by caffeine with respect to other stimulants such as amphetamine or cocaine.
In addition to caffeine in coffee, we can also find it in tea, cocoa and cola. The consumption of all these substances comes from antiquity. For example, about 4,700 years ago tea was consumed in China. The coffee plant, for its part, spread through Ethiopia, from where it passed to Arabia and India, probably thanks to the Muslim pilgrims who came to Mecca. However, the main coffee diffusers were the Dutch. In fact, from their colonies they took the first coffee plants to Europe and from there they extend to Guyana, Brazil and South America.
The cocoa made an inverse trip. The word cocoa comes from the Mayan language; Cach means red (cocoa shell color) and cau means strength and fire. As a result of the conquest of America, cocoa came to Europe, along with other new fruits. However, XIX. At the beginning of the twentieth century the development of the chocolate industry allowed the total expansion of cocoa consumption.
How does it affect the organism?
In general, caffeine is a stimulating or exciting substance. Therefore, it reduces fatigue and sleep and increases the ability to perform certain jobs. In high doses, caffeine can cause nervousness, restlessness, insomnia, tachycardia, diuresis, facial redness and alterations of the digestive system. In the intoxications produced by caffeine, muscle contractions, cardiac arrhythmias and psychomotor shaking may appear. However, all studies have shown that moderate consumption of caffeine does not produce toxic effects. In addition, unlike alcohol and nicotine, caffeine intake does not produce severe, long-term, and at average doses.

In the case of humans, taking coffee orally, the highest blood concentration of caffeine is reached at 30-45 minutes. The average life of caffeine (time needed to reduce blood concentration by half) is 3 hours in most cases, but it can be longer in newborns (due to the lower incidence of enzymes), contraceptive women, or in the first three months of pregnancy. In smokers, however, the average life of caffeine is reduced by 30-50%.
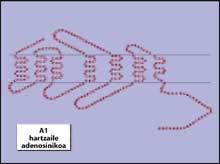
The most important effect of caffeine is to hinder the action of adenosine. Adenosine is an endogenous nucleoside that acts as a neuromodulator in various areas of the central nervous system. This nucleoside, activating its receptors (called adenosine receptors), slows the rhythm of neuronal excitation, decreasing synaptic transmission and releasing fewer neurotransmitters. Caffeine is an adenosine receptor antagonist, which hinders the effects of adenosine and favors synaptic transmission. Adenosine receptors A1 and A2 participate in the effects of caffeine. A1 receptors are distributed throughout the brain, but the largest amounts are concentrated in the hippocampus, talamo and skin of the brain and cerebellum. Those of the class A2a, on the contrary, are only found in the striated body, the nucleus accumbens and the olfactory bulb.
According to some studies, there is an interaction between A2a adenosine receptors and D2 dopaminergic receptors. The interaction between them of striated body can be responsible for some of the influences of methylxanthine in behavior. Adenosine makes activation of dopaminergic receptors difficult. Caffeine, therefore, as it antagonizes the effect of adenosine, favors dopaminergic neurotransmission. This mechanism, in addition to being related to certain physiological effects of caffeine, can also be responsible for dependence.
Uncontrolled search for caffeine
The World Health Organization (WHO) has published a list of requirements that must be met by subjects considered drugs to determine whether a substance produces or does not depend. Among these characteristics are the difficulty to leave the drug freely, the life around it, the withdrawal syndrome, tolerance and reinforcement.
Physical dependence
Abstinence syndrome and tolerance are the physical component of dependence. In animals, studies show that by suspending the administration of caffeine, clinical signs related to abstinence syndrome may appear. In fact, it seems that the abandonment of caffeine reduces both motor activity and booster behavior. Caffeine withdrawal syndrome depends on the dose and duration of treatment. The most obvious manifestation of the aforementioned clinical signs occurs in animals between 24 and 48 hours after the last dose of caffeine taken.
In humans, as well as in laboratory animals, there is a withdrawal syndrome. In this case there are clinical signs such as headache, weakness, sleep, depression, loss of concentration, difficulty working, fatigue, increased muscle tension and irritability. Normally, the most visible signs in the human being are manifested at 20-48 hours after the interruption of the administration of caffeine. However, in some individuals, abstinence syndrome may be more persistent or faster. Unlike animals, abstinence syndrome in humans seems not to be related to the amount of caffeine taken during the day.
It is known that many of the clinical signs that occur in abstinence syndrome are contrary to the effects of the drug itself in the body. Caffeine produces a forest contraction that reduces blood flow in the brain. In this sense, some studies have shown that the headache that appears in caffeine abstinence syndrome coincides with the increase in blood flow. In addition, it seems that women suffer more headache. Also, in old age, the headache that appears in the syndrome decreases. It should be noted that babies with fervent coffee growers can suffer from a withdrawal syndrome.
On the other hand, when tolerance to a drug occurs, the effects it can cause are reduced. Studies show that the chronic administration of caffeine, both in animals and humans, generates tolerance for certain effects. Tolerance for certain effects of caffeine on behavior occurs in animals, as is the case of the stimulation of motor activity. This tolerance occurs quickly and is crossed with other methylxanthines, but not with stimulants such as amphetamine. That is, if tolerance to caffeine occurs, in its composition tolerance to other drugs with a chemical structure of methylxanthine appears. Tolerance in animals is mainly based on biological changes that occur in the dopaminergic system and not on the number of adenosine receptors.
In humans, in a few days there is tolerance to certain physiological effects, such as increased blood pressure and heart rate, or increased plasma levels of adrenaline and noradrenaline. It is not clear whether tolerance to sleep alteration occurs. In fact, those who drink a lot of coffee suffer tolerance to insomnia that produces caffeine, but this tolerance is not complete. Therefore, in the human being, in terms of tolerance, the data collected so far are not as clear as those obtained in animals, and there seems to be great differences between people.
Is there psychic dependence on caffeine?
To answer this question for a long time, multiple views have arisen, often from personal experience and without evidence. According to the published scientific evidence, there are two types of studies: the epidemiological ones, that is, those that describe a population of consumers, and the experimental ones, that seek causes both in animals and in human beings controlling the design of the research and the requirements of its components.
Epidemiological studies
According to the study of Strain and its collaborators, of a sample of 16 people who met the criteria of dependence of the guide DSM-IV, 7 took refreshing drinks with caffeine, 8 took coffee and 1 took tea. The 75-94% of the sample claimed to have suffered on some occasion the abstinence syndrome or tolerance to caffeine, and 81-94% said they continued to take caffeine despite the damage and wanted to stop consuming caffeine. Therefore, we can say that caffeine generates physical and psychic dependence.
Experimental studies
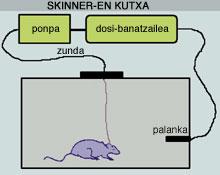
To know well the peculiarities of caffeine and other drugs, we must take into account the research carried out in laboratory animals. In the laboratory, to measure the dependence of drugs, a device called a Skinner box has been used. We place the animal in a small cage with lever, button or other handling system. This system at the disposal of the animal is associated with a device that supplies drugs, drugs or other solution. Thus, each time the animal acts on the lever it automatically receives a dose of this solution, usually intravenous, as a reward.
If the application of the first dose of the drug likes its effect, the animal learns to act again and again on the device, so we call this drug a booster boost. The effect of the solution, if you do not like it, stops activating the lever over time, called negative or neutral stimulus. The greater the efficiency of a booster stimulus, the more enthusiasm the animal has to continue acting on the lever, and then we say that the stimulus provokes self-administration. Self-administration has been taken as a model of human dependence and is used to predict whether the alleged drug produces dependency. Conventional drugs, such as amphetamine, cocaine and heroin, are very effective in the model of self-administration in all their species, types of animals and situations.
In the case of caffeine, the results have not been so clear. In some studies caffeine causes self-administration, while in other studies the capacity of caffeine reinforcement varies according to species and dose. In addition, with conventional drugs, the doses taken by the animal in the experiment gradually increase, but the self-administration of caffeine does not follow a gradual pattern. In fact, the animal takes caffeine from time to time, at high doses, from time to time and at low doses in others.
As for the dose, also in humans it has been shown that the amount of caffeine is important. In fact, although the amount of caffeine in cafes (25-50 mg) is sufficient for a boosting stimulation, as the dose of caffeine increases (400-600 mg) it becomes a negative or negligible stimulus. Finally, the self-administration of caffeine in humans depends on what everyone should do at that time. For example, with the availability of certain types of drugs, consumers choose caffeine-containing pills to carry out the task that requires attention. Therefore, although caffeine, like other drugs, is a boosting stimulus, it seems not as effective as amphetamine, cocaine, or heroin.
What is the biological basis of dependence?
The Russian Ivan Pavlov was the first researcher to study the influence of caffeine on behavior. Caffeine perceived that all stimuli, both rewarding and negative, reinforced the responses generated. These experiments, along with other later published studies, confirmed that caffeine acts as a stimulating drug in the central nervous system.

Thus, laboratory animals are able to learn to separate caffeine from the saline solution given to it, but they often confuse the effects of caffeine with those of stimulants (cocaine or amphetamines). Humans can also confuse the effects of caffeine with those of cocaine, at high doses, and intravenously. However, we cannot conclude that the dependence that produces caffeine and other drugs such as cocaine or heroin is equivalent.
Two hypotheses are known to explain why coffee cannot stop drinking coffee. According to the first theory, there is a negative reinforcement, that is, the chronic consumer must drink drinks with caffeine to avoid suffering from abstinence syndrome when it does not fall. One study has shown that people with headaches rarely leave coffee (headache is the most common symptom of abstinence).
According to the second theory called positive reinforcement, the chronic coffee maker tries to look for the pleasant effects of caffeine. And it is that the effects of caffeine are positive and attractive in humans, such as pleasure, germination, courage, passion for work and high self-esteem. Some researchers have announced that positive effects are more intense in low doses, especially if they are not chronic consumers.
What happens in our nervous system?
Drug use produces immediate cellular and molecular changes. If these changes occur chronically, the organism launches new mechanisms to maintain its balance. Although long-term changes can lead to dependency, we know little about it, and much less about caffeine.
The research carried out so far has analyzed only the actions of drugs and the acute effects to differentiate them from the mechanisms of drugs that are not drugs. Thus, it is very assumed that thanks to behavioral and neurophysiological studies, drugs activate in an acute way a certain neurobiological root, the mesolinvic system. This does not mean that other systems do not participate.
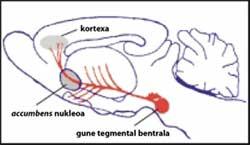
The mesolinbic system is also known as a network of awards, as it strengthens survival actions, such as food and sex as a reward. It is formed by dopaminergic neurons located in the ventral tegmental zone of the central nervous system, from which the pathways that lead to the nucleus accumbens and cortex leave. The awards network focuses on the response to booster stimuli and on motivational, rewarding and emotional functions.
Drugs such as cocaine, amphetamine, morphine, ethanol, cannabinoids and nicotine excite the dopaminergic system.
As for caffeine, until recently it has not been fully demonstrated that it provokes this type of dopaminergic mechanisms. In August 2002, Solinas and his companions showed that caffeine activates dopaminergic neurotransmission through the mesolinbic pathways.
Other researchers do not agree on these results, so they have proposed that caffeine only affects the mesolinic system with high doses that affect other central areas. In any case, it will be necessary to carry out more experiments in animals and humans (using other new techniques) to better understand the complicated mechanisms created by caffeine.
Caffeine in our dietMany of the foods we eat daily contain caffeine (coffee, tea, chocolate, cola drinks...). However, the amount of caffeine varies from one to the other, with coffee being the one that contains the most caffeine and the one that contains the least cola. In general, a daily average of 76 mg of caffeine has been estimated. However, this amount varies according to the country. The 55% of the caffeine that children drink comes from refreshing drinks, 35-40% chocolate products and the remaining 5-10% coffee or tea. In addition, a cup of caffeine can vary greatly depending on the preparation and type of coffee (Arabica or Robusta). According to all epidemiological studies, the global consumption of caffeine is increasing. In the impoverished regions, consumption of caffeine-containing foods has become an essential tool to deceive simple reinforcement or belly to address endless work sessions, while in the countries of the first world consumption has been based on the need for a stimulant to combat stress. The reflection of the latter is the appearance of energy drinks rich in caffeine. Among the ingredients of these drinks, in addition to caffeine itself, are other substances that are a source of caffeine, such as guaraní and cola. |
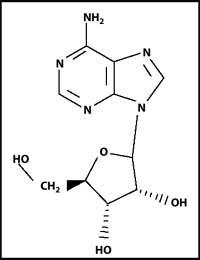
Chemical structure of caffeine
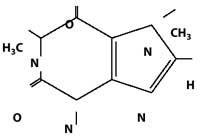
Caffeine was isolated in 1820. Chemically it is an alkaloid of the methylxanthine family (1,3,5-trimethylxanthine), the most important alkaloid of Caffea or Cacahuatl plants. As for tea, there has been some confusion, when its active component was isolated, it was called teina. However, the molecular study conducted years later revealed that theine was nothing more than caffeine. Among the scientists who have investigated the effects of caffeine we have several Nobel Laureates: Hermann Emil Fischer (Nobel Prize in Chemistry in 1902) and Hermann Staudinger (Nobel Prize in Chemistry in 1953).
BIBLIOGRAPHY BIBLIOGRAPHY
- Fredholm, B.B., Bättig, K., Holmén, J., Nehting, A. and Zvartau, E.E.Actions of caffeine in the brain with special reference to factors that contribute to its extended use.Pharmacol Rev 51 (1): 83-133. 1999 1999 1999
- Illy, E.•Research and Science 311: 68-74. 2002.
- A. Are we still dependent coffe and caffeine? A review on human and animal data.Neurosci Biobehav Rev 23: 563-576. 1999 1999 1999
- Solinas, M., Ferré, S., You, Z.-B., Karch-Kubicha, M., Popoli, P. and Goldberg, S.R.Caffeine induces dopamine and glutamate release in the shell of the nucleusaccumbens.J Neurosci 22 (15): 6321-6324. 2002.
- Strain, e.c., mumford, g., silverman, k. and griffiths, r.r.Caffeine dependence syndrome, evidence from case histories and experimental evaluations.
- JAMA 272 (13): 1043-1048. 1995.
Zu idazle
Zientzia aldizkaria

